FL CF-ES 2282 2006-2024 free printable template
Show details
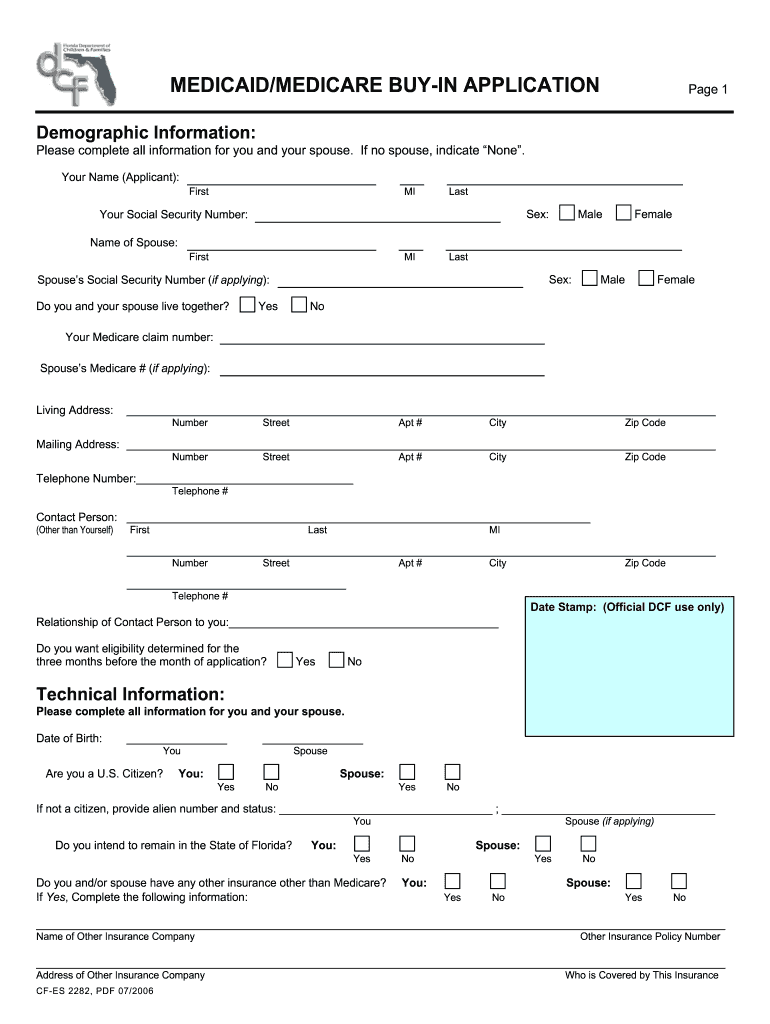
Save & Close Rename Cancel Clear Page 1 MEDICAID/MEDICARE BUY-IN APPLICATION Demographic Information: Please complete all information for you and your spouse. If no spouse, indicate e”. Your Name
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign

Edit your florida medicaid application form form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.

Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.

Share your form instantly
Email, fax, or share your florida medicaid application form form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit florida medicaid application form online online



Follow the guidelines below to take advantage of the professional PDF editor:
1
Create an account. Begin by choosing Start Free Trial and, if you are a new user, establish a profile.
2
Prepare a file. Use the Add New button to start a new project. Then, using your device, upload your file to the system by importing it from internal mail, the cloud, or adding its URL.
3
Edit florida medicaid application form. Add and change text, add new objects, move pages, add watermarks and page numbers, and more. Then click Done when you're done editing and go to the Documents tab to merge or split the file. If you want to lock or unlock the file, click the lock or unlock button.
4
Get your file. Select your file from the documents list and pick your export method. You may save it as a PDF, email it, or upload it to the cloud.
pdfFiller makes dealing with documents a breeze. Create an account to find out!
How to fill out florida medicaid application form

How to fill out florida medicaid application form?
01
Gather all necessary documents and information: Before starting the application, make sure you have all the required documents and information readily available. This may include identification documents, proof of income, proof of residency, Social Security numbers, and medical records.
02
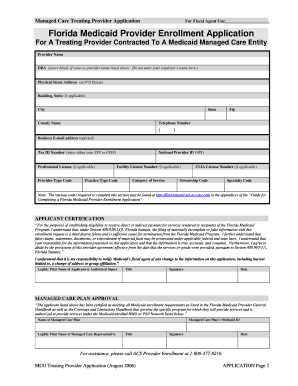
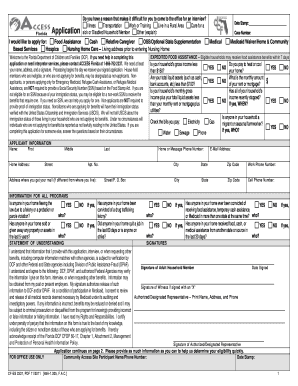
Access the application form: Visit the official website of the Florida Department of Children and Families or contact your local Department of Children and Families office to obtain a copy of the florida medicaid application form. You may also be able to complete the application online.
03
Fill out personal information: Begin by providing your personal details such as your name, address, date of birth, and contact information. Make sure to fill out all the required fields accurately.
04
Provide income and financial information: Provide information regarding your income, assets, expenses, and any other financial details requested in the application form. This may include details about your employment, self-employment, unearned income, and any financial resources you possess.
05
Include household information: If you are applying for Medicaid as a family or household, include information about other household members, including their names, ages, relationships to you, and their income details if applicable.
06
Fill out the medical information section: Include information about your health conditions and medical needs in the application form. This may include details about medical professionals you visit, prescription medications, and any disabilities or chronic illnesses you may have.
07
Review and double-check the application: Before submitting the application, thoroughly review all the filled out information to ensure accuracy and completeness. Any incorrect or missing information could potentially delay the processing of your application.
Who needs florida medicaid application form?
01
Individuals in Florida who meet the eligibility criteria for Medicaid and require financial assistance for their healthcare needs.
02
Families in Florida who meet the eligibility criteria for Medicaid and need healthcare coverage for their household members.
03
Individuals with disabilities or chronic illnesses in Florida who require financial assistance for their medical expenses and meet the Medicaid eligibility requirements.
Fill medicaid application florida pdf : Try Risk Free
People Also Ask about florida medicaid application form online
Why was i denied Medicaid in Florida?
How long does it take to get approved for Florida Medicaid?
What's the income limit for Medicaid in Florida?
How much do you need to qualify for Medicaid in Florida?
Can I apply for Medicaid in person in Florida?
What is required to apply for Medicaid in Florida?
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How to fill out florida medicaid application form?
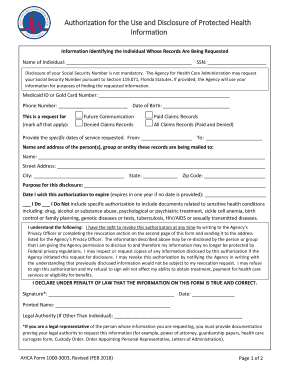
1. Visit the Florida Agency for Health Care Administration (AHCA) website to download the Medicaid application form.
2. Complete the form by filling in the required information. This includes personal information such as names, addresses, dates of birth, Social Security number and any other people in your household who are applying for Medicaid.
3. Provide information about your income, resources and assets. This includes employment, wages, bank accounts, stocks, bonds, and other assets.
4. Attach proof of income, such as pay stubs, Social Security statements or tax returns.
5. Sign and date the application.
6. Submit the application either by mail or online. The mailing address is on the form. If you are submitting it online, there is a link on the form that will take you to the AHCA website.
What is the purpose of florida medicaid application form?
The Florida Medicaid application form is used to determine if an individual is eligible to receive Medicaid services in the state of Florida. It collects information about the applicant's income, household size, and other factors to determine eligibility.
What information must be reported on florida medicaid application form?
The Florida Medicaid application form requires information about the applicant's identity, income and financial resources, household size, health care coverage, and other information needed to determine eligibility. Applicants are also required to provide proof of Florida residency, Social Security number, and any income-related documents.
What is florida medicaid application form?
The Florida Medicaid application form is the official document that individuals must complete and submit in order to apply for Medicaid benefits in the state of Florida. This form collects important personal and financial information, as well as details about the applicant's household and medical needs, to determine eligibility for Medicaid services. The application form is available online on the Florida Department of Children and Families website, or can be obtained by visiting a local Medicaid office.
Who is required to file florida medicaid application form?
Anyone who meets the eligibility requirements for Florida Medicaid is required to file a Medicaid application form. This typically includes low-income individuals and families, pregnant women, children, disabled individuals, and seniors who meet certain income and asset criteria. Additionally, it is necessary to reapply and renew Medicaid benefits on a regular basis to maintain eligibility.
What is the penalty for the late filing of florida medicaid application form?
There is no specific penalty outlined for the late filing of a Florida Medicaid application form. However, it is generally recommended to submit the application as soon as possible to avoid any delays in receiving benefits. If the application is not submitted within a reasonable period of time, it may result in a delay in eligibility determination and the start of Medicaid coverage.
How can I manage my florida medicaid application form online directly from Gmail?
florida medicaid application form and other documents can be changed, filled out, and signed right in your Gmail inbox. You can use pdfFiller's add-on to do this, as well as other things. When you go to Google Workspace, you can find pdfFiller for Gmail. You should use the time you spend dealing with your documents and eSignatures for more important things, like going to the gym or going to the dentist.
Where do I find florida medicaid application form pdf?
With pdfFiller, an all-in-one online tool for professional document management, it's easy to fill out documents. Over 25 million fillable forms are available on our website, and you can find the medicaid application florida in a matter of seconds. Open it right away and start making it your own with help from advanced editing tools.
Can I create an eSignature for the medicaid application form florida in Gmail?
It's easy to make your eSignature with pdfFiller, and then you can sign your florida medicaid application form right from your Gmail inbox with the help of pdfFiller's add-on for Gmail. This is a very important point: You must sign up for an account so that you can save your signatures and signed documents.
Fill out your florida medicaid application form online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Florida Medicaid Application Form Pdf is not the form you're looking for?Search for another form here.
Keywords relevant to printable medicaid application form
Related to medicaid medicare buy in form






If you believe that this page should be taken down, please follow our DMCA take down process
here
.
